Article Text

Abstract
Objective This study aimed to assess whether additional enteral docosahexaenoic acid (DHA) supplementation, with or without arachidonic acid (ARA), influences morbidities diagnosed in the neonatal intensive care unit among preterm infants, excluding administration via formula or parenteral nutrition.
Design and setting This meta-analysis involved a comprehensive search of the PubMed, Embase, Web of Science and Cochrane Library databases from their inception to 9 June 2024.
Patients and interventions Randomised controlled trials focusing on the effects of enteral DHA with or without ARA in preterm infants born at ≤34 weeks gestational age or a birth weight ≤2000 g were included.
Main outcomes and measures The main outcomes included in-hospital mortality, bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotising enterocolitis (NEC), sepsis, intraventricular haemorrhage (IVH) and periventricular leukomalacia (PVL).
Results Eleven trials evaluating distinct adverse outcomes in preterm infants were incorporated. Of these, nine trials assessing enteral DHA supplementation with or without ARA indicated an increased risk of BPD with a relative risk of 1.11 (95% CI 1.00 to 1.22). Additionally, five trials assessing DHA supplementation without ARA showed an increased risk of BPD with a relative risk of 1.15 (95% CI 1.03 to 1.28). No significant effects were observed on the incidence of ROP, NEC, sepsis, IVH, PVL or in-hospital mortality.
Conclusions and relevance Enteral supplementation of DHA with or without ARA did not demonstrate protective effects against major complications in preterm infants and even increased the risk of BPD. Further research is warranted to evaluate the necessity of DHA and ARA supplementation in this population.
PROSPERO registration number CRD42024552578.
- Neonatology
- Intensive Care Units, Neonatal
- Micronutrients
- Primary Health Care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Premature birth disrupts the natural maternal supply of essential fatty acids, such as docosahexaenoic acid (DHA) and arachidonic acid (ARA), which are critical for the optimal development of preterm infants.
Preterm infants usually face a high risk of complications, and exogenous supplementation of DHA and ARA is recommended to improve their outcomes.
WHAT THIS STUDY ADDS
Enteral supplementation of DHA with or without ARA did not demonstrate protective effects against major complications like retinopathy of prematurity, NEC, sepsis, intraventricular haemorrhage, periventricular leukomalacia, or in-hospital mortality in preterm infants and even increased the risk of bronchopulmonary dysplasia (BPD).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given the lack of demonstrated benefits and potential risks, particularly the increased risk of BPD, the necessity and timing of enteral DHA and ARA supplementation in preterm infants should be reconsidered and further investigated.
Introduction
Preterm birth significantly impacts neonatal health, leading to adverse outcomes and placing a considerable burden on families and society.1 Due to their immaturity, preterm infants frequently encounter complications during hospitalisation, including bronchopulmonary dysplasia (BPD), retinopathy of prematurity (ROP), necrotising enterocolitis (NEC), sepsis, intraventricular haemorrhage (IVH) and periventricular leukomalacia (PVL), substantially heightening the risk of adverse outcomes. Among the array of supportive interventions for preterm infants, optimising ex utero nutrition as a scientific substitute for in utero nutrient provision is paramount for mitigating the risk of multiple systemic complications and ensuring optimal growth and development.
In clinical practice, polyunsaturated fatty acids (PUFAs) play a pivotal role as essential nutrients, available through breast milk, formula milk, intravenous lipid emulsions and additional single commercial products.2 Linoleic acid and alpha-linolenic acid are essential fatty acids that require exogenous intake. Docosahexaenoic acid (DHA) and arachidonic acid (ARA), representing n-3 and n-6 PUFAs, respectively, are downstream metabolites of linoleic acid and alpha-linolenic acid, which can be synthesised endogenously or supplemented exogenously. DHA is crucial for brain development, visual acuity and cardiovascular health, while ARA plays a significant role in the inflammatory response, immune function and cell membrane integrity. In recent years, exogenous supplementation of DHA and ARA, through single commercial products, has been extensively employed in clinical settings, with the anticipation of mitigating early adverse outcomes and ensuring favourable long-term neurological prognosis in preterm infants.3 4
Nevertheless, the latest systematic reviews evaluating the impact of DHA supplementation through a combination of dietary intake, intravenous lipid emulsions and additional commercial products have shown that augmenting DHA with or without ARA or other PUFAs does not significantly reduce the risk of ROP,5 6 and single DHA supplements may even elevate the risk of NEC.7 The findings regarding BPD are inconclusive: while DHA with or without ARA supplementation does not increase the risk, high doses of DHA may increase the incidence of BPD.8–11 The above studies suggest that additional DHA supplementation, with or without ARA, may not be necessary. However, these studies primarily focused on a single specific condition. More importantly, the interventions in these studies included not only oral supplementation but also additional DHA or ARA administered through formula or parenteral nutrition. These two methods differ significantly in dosage, with enteral formulations uniquely increasing both the workload for healthcare providers and the financial burden on patients.
This study seeks to investigate the necessity of extra DHA supplementation, with or without ARA, in preterm infants by clarifying the association between singular enteral DHA supplementation with or without ARA and adverse outcomes in preterm infants through systematic review and meta-analysis, furnishing a theoretical foundation for the clinical application of DHA and ARA.
Methods
The study was conducted following Cochrane Handbook procedures (V.5.1.0) and Cochrane Neonatal Review Group guidelines (https://training.cochrane.org/handbook/archive/v5.1/). Reporting was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines.12 The protocol was registered with PROSPERO (CRD42024552578).
Eligibility criteria
We included randomised controlled trials focusing on preterm infants, primarily those born with a gestational age of less than 34 weeks or a birth weight of less than 2000 g, regardless of maternal supplements either before or after birth. Conference abstracts, reviews and case reports were not included.
In the intervention group, infants received enteral DHA with or without ARA within 28 days of birth, while the control group received either placebo or no intervention. Studies involving enhanced DHA with or without ARA in formula or lipid emulsions were excluded. There were no specific requirements for the dosage and duration of intervention.
Outcome measures focused on early complications in preterm infants, including BPD, ROP, NEC, sepsis, IVH, PVL and in-hospital mortality. These outcomes were assessed whether reported as primary or secondary outcomes in the included studies. The diagnostic criteria for diseases were not restricted and are detailed in online supplemental table 1.
Supplemental material
Data sources and search strategy
The literature search was performed using databases including PubMed, Embase, Web of Science and Cochrane library from the inception of each database to 9 June 2024. The search strategy used both Medical Subject Headings and text words. Detailed search strategies for each database are provided in the online supplemental appendix 1. Duplicate records across databases were removed using ENDNOTE software.
DD and ZG independently screened titles, followed by abstracts, and finally full-text articles, to determine eligibility for inclusion. Additionally, we also manually searched the reference lists and bibliographies of included studies to identify additional relevant reports.
Data extraction and risk-of-bias assessment
DD and ZG independently extracted data from the included articles to ensure accuracy and reliability. In cases where there was disagreement over the extracted data, CZ acted as an arbiter to resolve the discrepancies and determine the final data. The data extraction process involved collecting information on the study author, study country, study year, sample size, participants (gestational age/birth weight), supplement intervention, placebo, start time of intervention, duration of interventions, and adverse outcomes of preterm infants. For assessing the risk of bias, the Cochrane risk-of-bias tool was employed.
Data synthesis and statistical analysis
Analysis was conducted using Review Manager V.5.4 (Cochrane Collaboration, Nordic Cochrane Centre, Copenhagen, Denmark) with a fixed-effects model and the Mantel-Haenszel method for categorical variables. Effect sizes were estimated as risk ratios (RRs) for treatment along with 95% CIs for each outcome. Between-study heterogeneity of the effect estimates was assessed by inspecting forest plots and calculating I2 statistics. In cases of notable heterogeneity (I2>50%), potential sources were investigated. Sensitivity analysis was conducted by analysing data according to different disease severity outcomes, including moderate to severe BPD,13 14 requiring therapy ROP, grade III-IV IVH, and confirmed NEC defined as Bell stage II or higher.15 16 Additional subgroup analyses were conducted based on DHA alone (DHA group) and DHA combined with ARA (DHA&ARA group), as well as varying DHA dosages, with high-dose DHA defined as >60 mg/kg/day. Funnel plots were used to assess publication bias. A two-sided value of p<0.05 was considered statistically significant.
Quality assessment of pooled analysis
We used the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) system17 to assess the quality of evidence for each unique pooled analysis, categorising them as ‘high’, ‘moderate’, ‘low’ or ‘very low’. Of the eight criteria established by the GRADE method, five—risk of bias, inconsistency of results across studies, indirectness of evidence, imprecision and publication bias—can undermine confidence in the accuracy of effect estimates, which may lead to downgrading.
Results
Trial selection and characteristics
We initially identified a total of 9707 relevant articles through our comprehensive search strategy. After applying our inclusion and exclusion criteria, 19 articles were thoroughly evaluated. We excluded one article18 due to the absence of outcome variables and four articles19–22 due to duplicate data from the same studies. Consequently, data from 14 articles23–36 representing 11 unique trials were included (figure 1).

Flow chart of search results.
These 11 trials encompassed a cohort of 2567 preterm infants from 10 different countries. Detailed study characteristics are provided in table 1. Specifically, 9 studies focused on BPD, 8 studies addressed ROP, 10 focused on NEC, 8 on sepsis, 7 on IVH, 4 on PVL and 4 on in-hospital mortality. The dosages of DHA varied across studies from 20 mg/kg/day to 1.2 g/day, and ARA dosages from 40 mg/kg/day to 240 mg/kg/day. The intervention typically began within the first 7 days of life and continued for 14 days, up to 36 weeks or 40 weeks of corrected gestational age, or until discharge.
Characteristics of included studies
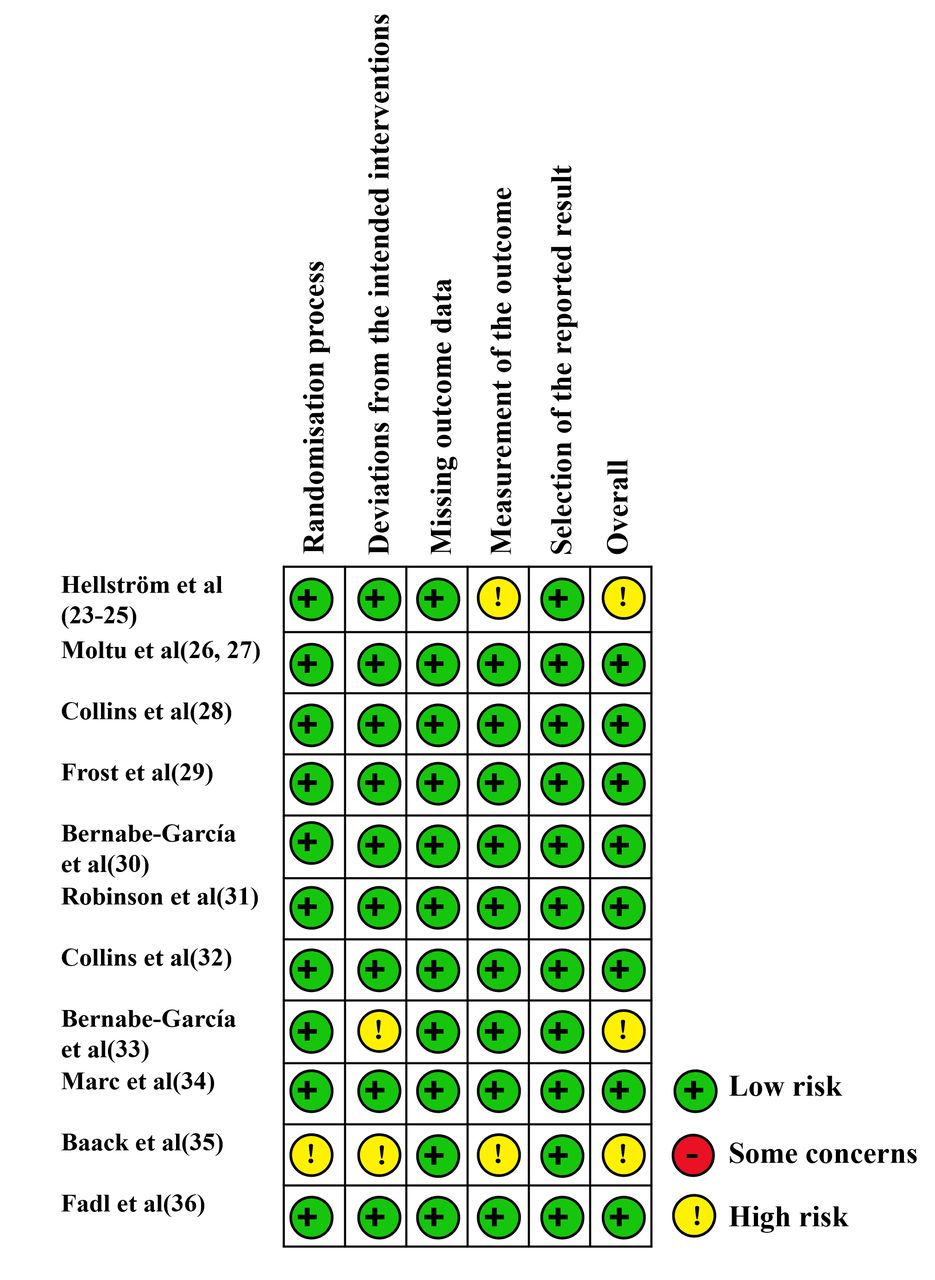
Among the 11 included trials, 323 33 35 were assessed as having some concerns regarding bias, while 826–32 34 36 were considered to have a low risk of bias. No studies were identified as having a high risk of bias (figure 2). Funnel plot demonstrated no evidence of significant publication bias (online supplemental figure 1).

{kind=link}
{kind=link}
Risk-of-bias assessment of individual trials.
Data synthesis on complications in preterm infants
A comprehensive data synthesis analysis was performed to evaluate the impact of enteral DHA with or without ARA supplementation on the risk of early complications in preterm infants, including BPD, ROP, NEC, sepsis, IVH, PVL and in-hospital mortality (table 2 and online supplemental figure 2.1–2.7). The findings revealed varied effects of DHA with or without ARA on these conditions. Notably, the analysis of nine studies23 26 28–32 34 35 encompassing 2272 infants indicated an increased risk of BPD associated with supplementation (RR: 1.11; 95% CI 01.00 to 1.22; I2=0). Meanwhile, five studies23 26 30 33 34 on any ROP found no significant link between DHA with or without ARA and the occurrence of ROP (RR: 0.96; 95% CI 0.84 to 1.10; I2=0). The pattern of no significant association continued with other complications: 10 studies23 26 28 29 31–36 involving 2457 infants showed no correlation with NEC (RR: 1.00; 95% CI 0.74 to 1.33; I2=7%), 8 studies23 26 28–31 34 35 involving 2244 infants found no link with sepsis (RR: 0.95; 95% CI 0.85 to 1.06; I2=20%), and 7 studies24 26 28 29 31 34 35 involving 2245 infants reported no connection with IVH (RR: 1.03; 95% CI 0.91 to 1.16; I2=21%). Similarly, four studies26 28 34 35 involving 1866 infants demonstrated no relationship with PVL (RR: 0.76; 95% CI 0.39 to 1.49; I2=0). Lastly, the analysis of four studies23 28 34 35 including 2060 infants indicated that DHA with or without ARA did not affect in-hospital mortality rates (RR: 1.11; 95% CI 0.83 to 1.49; I2=53%). Overall, while DHA with or without ARA appears to increase the risk of BPD, it shows no significant impact on other major complications in preterm infants.
Enteral supplementation of DHA with or without ARA and adverse outcomes in preterm infants
Subgroup analyses
Analyses of the stratified subgroups revealed an increased risk of BPD in preterm infants in the DHA group (RR: 1.15; 95% CI 1.03 to 1.28; I2=0). However, the risk of BPD did not increase in the DHA&ARA group, and no correlation was observed between the DHA or DHA&ARA groups and the occurrence of ROP, NEC, sepsis, IVH, PVL, or in-hospital death (table 3 and online supplemental figure 2.1–2.7).
Subgroup and sensitivity analyses of DHA with or without ARA supplementation on adverse outcomes in preterm infants
Analyses of the stratified groups based on high-dose and low-dose DHA with or without ARA revealed that the risk of BPD increased in the high-dose DHA group (RR: 1.27; 95% CI 1.02 to 1.60; I2=0). Although the low-dose group did not show a statistically significant increase, there was a clear trend towards higher risk (RR: 1.06; 95% CI 0.96 to 1.18; I2=0). No correlation was observed between DHA dosage and the occurrence of ROP, NEC, sepsis, IVH, PVL or in-hospital death (table 3 and online supplemental figure 3.1–3.7).
Sensitivity analyses
Analyses of stratified subgroups focusing on the severity of diseases in preterm infants who received DHA with or without ARA revealed the following: supplementation with DHA with or without ARA increased the risk of moderate-to-severe BPD (RR: 1.11; 95% CI 1.00 to 1.24; I2=0). There was no correlation between DHA supplementation and the occurrence of ROP requiring therapy, Bell stage II or higher NEC or grade III-IV IVH (table 3 and online supplemental figure 4.1–4.4).
Discussion
This study systematically reviewed the relationship between enteral DHA with or without ARA and various complications in preterm infants. Unfortunately, the findings revealed that, while there was no increased risk of mortality, ROP, NEC, sepsis, IVH or PVL, the expected protective effects against these conditions were also not observed. Furthermore, the supplementation even increased the risk of BPD, challenging the clinical application of enteral DHA and ARA in preterm infants.
In contrast to previous meta-analyses, this study uniquely focuses on preterm infants as the primary subjects of investigation and examines the effects of enteral supplementation specifically involving DHA with or without ARA. This sets it apart from earlier research efforts that amalgamated interventions, such as prenatal or postnatal supplementation in preterm mothers, increased dose of DHA or ARA in formula milk, or modifications in lipid emulsion content, which were not strictly enteral supplementation. The objective of this study is to provide a clear understanding of the clinical benefits or potential risks associated with additional enteral supplementation in preterm infants.
Prior systematic reviews have revealed divergent findings concerning the impact of DHA with or without ARA supplementation on the incidence of BPD in mothers or preterm infants receiving elevated doses via oral, formula or intravenous lipid emulsions. While some reviews indicate no significant correlation with BPD occurrence,8 10 11 one study hints at a potential heightened risk associated with high doses of DHA.9 However, our study aligns with recent meta-analytical evidence indicating that enteral high-dose DHA with or without supplementation may elevate the risk of BPD. Notably, we also observed a concerning trend towards increased BPD risk in the low-dose DHA group, with a calculated RR of 1.06 (95% CI 0.96 to 1.18). Potential mechanisms underlying the observed heightened BPD risk associated with DHA supplementation warrant exploration. Given DHA’s classification as a type of PUFA, it is conceivable that supplementation may augment the production of lipid peroxides and other oxidative stressors,37 contributing to pulmonary injury and inflammation. Furthermore, despite DHA’s recognised anti-inflammatory properties, supplemental intake may disrupt the delicate equilibrium between anti-inflammatory and proinflammatory pathways,38 thereby exacerbating lung injury and predisposing to BPD development.
In the context of NEC, previous studies have suggested that DHA supplementation alone increases the risk of NEC, while the combination of DHA and ARA appears to reduce this risk.7 However, our study suggests that no protective or harmful effects were observed with either singular or combined supplementation. Our findings also did not reveal a protective effect against NEC onset, as reported in the animal study.39 Consistent with previous meta-analyses on ROP,5 6 our investigation indicates that enteral supplementation of DHA with or without ARA fails to mitigate the risk of ROP or the necessity for treatment. Additionally, we found no significant correlation between enteral supplementation of DHA with or without ARA and the occurrence of IVH, PVL, sepsis or death, which has been rarely reported previously.
Some researchers posit that exclusive DHA supplementation may perturb the delicate balance of n-3 and n-6 PUFAs metabolism,40 potentially culminating in adverse outcomes. They advocate for combined DHA and ARA supplementation to uphold PUFA homoeostasis and avert the onset of diseases. Nevertheless, our study indicates that combined administration of DHA and ARA does not confer a reduced risk of adverse outcomes among preterm infants.
Based on our study findings and recent assessments, the clinical utilisation of DHA and ARA warrants re-evaluation. DHA and ARA, as vital components of neuronal and photoreceptor cell membrane phospholipids, were initially intended to enhance neurological and visual development. However, two crucial considerations emerge: first, our study indicates that enteral supplementation of DHA and ARA, as well as recent practices of fortifying DHA and ARA through formula feeding or intravenous nutrition, did not ameliorate the risk of early complications in preterm infants. Second, existing research suggests that supplementing with DHA and ARA does not yield significant improvements in neurological outcomes for preterm infants.41 42 Henceforth, given the risks of early onset diseases, the substantial expense of these products, and the increased workload for healthcare providers associated with administering medications, the necessity and timing of DHA and ARA supplementation in preterm infants merit further investigation.
The study possesses several limitations. First, in this meta-analysis, variations in DHA and ARA dosage and duration may have influenced the generalisability of the results and the ability to draw definitive conclusions. Second, discrepancies in the definition of outcomes for preterm infants across the included studies may have hampered data integration and result comparability. Third, there is a lack of clarity regarding the type of intravenous lipid emulsion administered, if any, as well as insufficient information about the composition of the enteral lipid emulsions, which may contain other fatty acids, although in smaller amounts. Additionally, the ratio of DHA to ARA warrants further analysis. Lastly, it is noteworthy that the baseline levels of DHA and ARA in the study subjects, encompassing preintervention, during intervention and postintervention phases, were inadequately delineated. Some studies suggest that high levels of DHA with or without ARA are associated with a lower risk of BPD.19 The ambiguity in the baseline levels of DHA engenders uncertainties regarding whether the additional supplementation adequately compensated for any deficiency, whether exogenous supplementation disrupted normal metabolism, or even led to potential oversupplementation. Addressing these uncertainties should constitute a priority for future research endeavours.
Conclusions
The study systematically reviewed the association between enteral supplementation of DHA, with or without ARA, and various complications in preterm infants. While no benefits were observed in improving outcomes related to mortality, BPD, ROP, NEC, sepsis, IVH and PVL, the anticipated protective effects were also not evident. In fact, under specific conditions, DHA supplementation was found to increase the risk of BPD. Therefore, considering the lack of demonstrated benefits, alongside the potential risks and economic burden, further investigation into both the necessity and optimal timing of DHA and ARA supplementation in preterm infants is warranted.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Footnotes
Contributors HW is the guarantor. DD: study concept and design, development of methodology, analysis and interpretation of data, writing of the original draft, read and approved the final paper. ZG: study concept and design, technical and material support, read and approved the final paper. CZ: technical support, read and approved the final paper. XM and XL: analysis and interpretation of data, statistical analysis, read and approved the final paper. HW: study concept and design, project administration, writing of the review and editing, read and approved the final paper.
Funding This study was funded by the National Natural Science Foundation of China (82271737, 82301952); Jilin Provincial Department of Science and Technology (YDZJ202301ZYTS070, 20130402013GH, YDZJ202501ZYTS670).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.