Article Text

Abstract
Objective Despite lack of evidence supporting efficacy, prophylactic fresh frozen plasma and Octaplas transfusions may be administered to very preterm infants to reduce bleeding risk. International variation in plasma transfusion practices in neonatal intensive care units (NICUs) is poorly understood, therefore, we aimed to describe neonatal plasma transfusion practice in Europe.
Design Prospective observational study.
Setting 64 NICUs in 22 European countries, with a 6-week study period per centre between September 2022 and August 2023.
Patients Preterm infants born below 32 weeks of gestational age.
Interventions Admission to the NICU.
Main outcome measures Plasma transfusion prevalence, cumulative incidence, indications, transfusion volumes and infusion rates and adverse effects.
Results A total of 92 of 1143 infants included (8.0%) received plasma during the study period, collectively receiving 177 transfusions. Overall prevalence was 0.3 plasma transfusion days per 100 admission days, and rates varied substantially across Europe. By day 28 of life, 13.5% (95% CI 10.0% to 16.9%) of infants received at least one plasma transfusion, accounted for competing risks of death or discharge. Transfusions were given for a broad range of indications, including active bleeding (29.4%), abnormal coagulation screen results (23.7%) and volume replacement/hypotension (21.5%). Transfusion volumes and infusion rates varied significantly; the most common volume was 15 mL/kg (range: 5–30 mL/kg) and the most common duration was 2 hours (range: 30 min to 6 hours).
Conclusions We found wide variation in plasma transfusion practices in Europe, highlighting the need for evidence to inform neonatologists in daily practice and guidelines, in particular for non-bleeding indications.
Trial registration number ISRCTN17267090.
- Neonatology
- Intensive Care Units, Neonatal
- Epidemiology
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Considerable uncertainty exists about the optimal use of plasma transfusions in very preterm infants. Plasma may be beneficial in a clinical setting with active bleeding and abnormal coagulation, although there is limited direct evidence in neonates.
WHAT THIS STUDY ADDS
We observed considerable variation in plasma transfusion practices across Europe, with many transfusions given for indications which are not sufficiently evidence based. Transfusion use, volume and infusion rate of plasma transfusions varied widely across European countries.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results underline the need for evidence-based strategies to guide plasma transfusion use in intensive care for very preterm infants, specifically for non-bleeding indications.
Introduction
Considerable uncertainty exists about the optimal use of plasma transfusion in very preterm infants born below 32 weeks of gestation. Fresh frozen plasma (FFP) or Octaplas transfusion may be beneficial in a clinical setting with active bleeding and abnormal coagulation, although there is limited direct evidence in neonates.1–3 However, plasma transfusions are also used in the neonatal intensive care unit (NICU) for other indications with very little evidence of benefit, including for abnormal coagulation screen results alone in the absence of active bleeding or for fluid replacement.4 5 A single randomised controlled trial (RCT) published in 1996 assessed the effect of prophylactic plasma transfusion in very preterm infants and showed no reduced risk of cerebral ultrasound abnormalities and long-term outcomes (although it did not incorporate coagulation screening).6 7 In addition, observational studies have demonstrated that FFP transfusions often fail to correct abnormal coagulation screen results, particularly if abnormalities are minor.2 6 8 Finally, reference ranges used in NICU are frequently based on limited and historical studies, so assessing coagulopathy in preterm infants may not be straightforward.9–12 Despite this, a recent survey showed that 39% of European NICUs transfuse plasma to infants for abnormal coagulation screen results without active bleeding.13 A better understanding of current practices can help identify research priorities and promote more evidence-based practice for preterm infants in the future. Recognising the current knowledge gap, we performed a prospective observational study describing plasma transfusion practices including plasma transfusion prevalence and incidence, primary indications for transfusion, transfusion volumes and infusion rates across 64 NICUs in 22 European countries.
Methods
Study design
We performed an international, prospective, observational cohort study (International Neonatal Transfusion Point Prevalence study) to evaluate current red blood cell (RBC), platelet and plasma transfusion practices in preterm infants in Europe. RBC and platelet transfusion data are published in separate articles.14 15
National coordinating clinicians led the recruitment of participating tertiary-level NICUs in their country. We invited a number of centres per country proportional to the population size of each country relative to other participating countries. In collaboration with the European Foundation for the Care of the Newborn Infant, a parent advisory board provided input in every stage of the study. We enrolled the study protocol (online supplemental file 2) in the ISRCTN registry (ISRCTN17267090). We conducted the study in accordance with the General Data Protection Regulation and Declaration of Helsinki. We followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline.
Supplemental material
Study participants and data collection
Study protocol included all very preterm infants born below 32 weeks of gestation who were admitted to one of the participating NICUs during the 6-week study period. Parents or guardians provided consent where required by national or regional legislation. We included preterm infants on NICU admission, date of consent or start of the study period, whichever came last. We continued study observation period until earliest of the following time points: day of death, day of discharge or last day of the study period.
Data collection
All participating centres collected data over a 6-week study period between September 2022 and August 2023. We defined a transfusion event as administration of a plasma transfusion. This was primarily FFP and Octaplas. For each plasma transfusion event, we collected the type of transfusion, primary indication, volume and duration of transfusion. Primary indications for transfusion could be selected from a predefined option list, including active bleeding, abnormal clotting test(s), prevention of major bleeding, surgical procedure, volume replacement/hypotension, sepsis and other. We also collected any adverse effects that neonatologists considered to be possibly related to the transfusion using a yes/no question, followed by a free text commentary. In the absence of clear definitions of transfusion-associated adverse effects in preterm infants, we opted for a free text format with the aim of gaining insights in adverse effects neonatologists identify in clinical practice.
Additionally, we documented instances of major bleeding, culture-positive sepsis, necrotising enterocolitis (NEC), invasive mechanical ventilation and surgery, with definitions provided in online supplemental eTable 1. We collected study data with a validated electronic Castor database that adhered to standards of ICH E6 Good Clinical Practice.
Supplemental material
Although we also collected information on the use of cryoprecipitate, we reported the use of cryoprecipitate separately from plasma transfusions in the Results section because it differs from FFP and Octaplas. Cryoprecipitate is derived from further processing of FFP, making it a more concentrated source of fibrinogen, von Willebrand factor, and factors VIII and XIII. Clinical use of cryoprecipitate also varies from that of FFP and Octaplas, as it is primarily indicated to replace fibrinogen, for which fibrinogen concentrate is used in many European countries instead.
Outcome measures
The main outcome measures of the study comprised (1) the plasma transfusion day prevalence rate, (2) the patient-mix adjusted plasma transfusion day prevalence rate and (3) the cumulative incidence of receiving at least one plasma transfusion within the first 28 postnatal days of life. A plasma transfusion day was defined as any admission day in the study period on which the infant received at least one plasma transfusion. Plasma transfusion day prevalence rate was defined as the number of plasma transfusion days per 100 NICU admission days, hereafter referred to as plasma transfusion prevalence. For the cumulative incidence, we only included infants enrolled from day of birth and accounted for competing risks of death and discharge. Additional study outcomes included primary indications for plasma transfusion, transfusion volume, duration, and infusion rate, and transfusion-related adverse effects.
Statistical analysis
We drafted a statistical analysis plan prior to conduct of the analysis (online supplemental file 4). We presented patient and centre characteristics as median (IQR) or frequencies (%).
Supplemental material
For the main study outcome measures, we calculated the overall plasma transfusion prevalence by pooling estimates from individual centres into subgroup estimates per country, which were then combined into the overall estimate using random effects Poisson models.16 Additionally, to calculate patient-mix adjusted prevalences per country, we developed a logistic regression with transfusion day (yes/no) as the dependent variable, and sex, gestational age at birth, birth weight, congenital malformations, major bleeding, NEC, sepsis, mechanical ventilation, surgical procedure and postnatal day as independent variables. We subsequently used this model to predict plasma transfusion per day for all individual infants in the study and averaged these predictions to derive the expected prevalence per country. Subsequently, the observed transfusion prevalence was divided by expected prevalence per country. Finally, we multiplied these country-specific observed/expected ratios by the overall observed prevalence to derive the patient-mix adjusted prevalence. For the computation of the cumulative incidence of receiving at least one plasma transfusion during the first 28 days of life, we considered death and discharge as competing events and we only included infants who were followed from birth. We conducted the analysis of the main study outcome measures using R statistical software (V.4.1.17, R Core Team, 2021), with function ‘metarate’ from package ‘meta’ and function ‘cuminc’. We performed computations for the remaining study outcome measures in STATA statistical software (V.16.1, Texas, USA). We computed transfusion infusion rates (mL/kg/hour) by dividing transfusion volume (mL/kg) by transfusion duration (hours). Figures were made using GraphPad Prism (V.9.3.1, California, USA).
Results
Patients and centres
We enrolled a total of 1143 patients from 64 NICUs in 22 European countries. Patient characteristics are presented in table 1. Infants included in the study had a median gestational age at birth of 28+2 weeks (IQR: 26+2 to 30+2 weeks) and a median birth weight of 1030 g (IQR: 780–1350 g). Median study observation period per infant was 20 days (IQR: 10–35), resulting in a total of 24 978 study days. We presented centre characteristics in online supplemental eTable 2.
Patient characteristics
Plasma transfusion
In total, 92 patients (92/1143, 8.0%) received one or more plasma transfusions during the study period, collectively receiving 177 transfusions. Median number of plasma transfusions per transfused infant was 1 (IQR: 1–2). Nearly all were FFP transfusions (175/177, 98.9%), two were Octaplas (2/177, 1.1%). In 151 of 177 (85.3%) plasma transfusions, the infant received invasive mechanical ventilation during the transfusion.
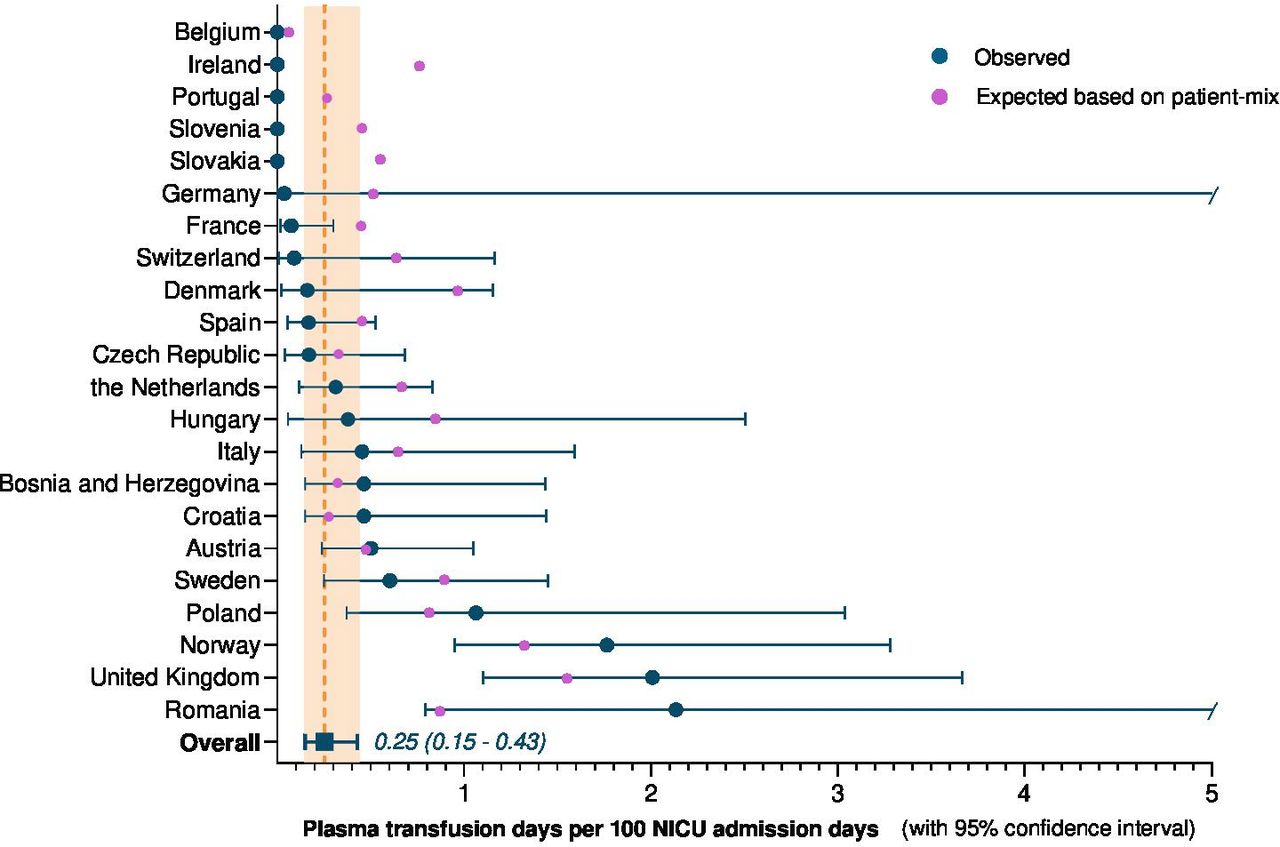
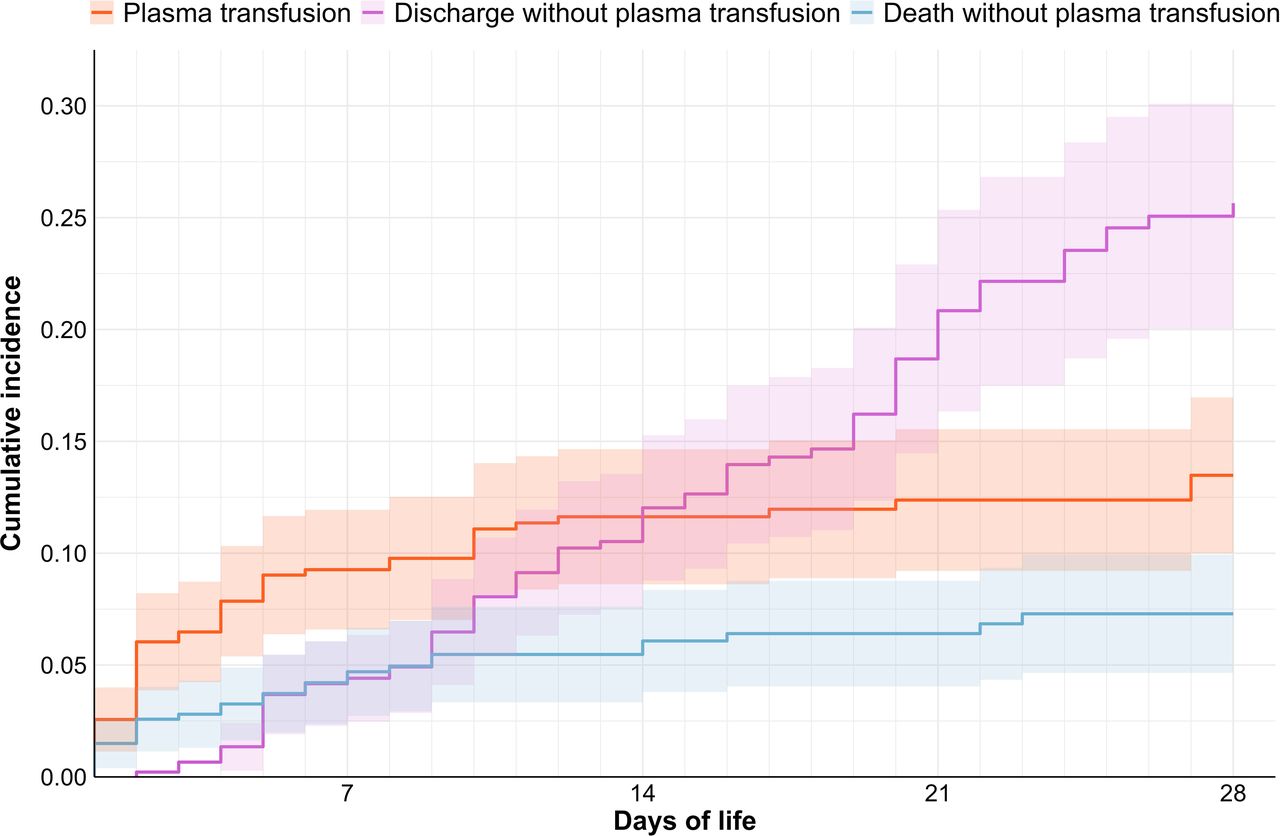
The overall plasma transfusion prevalence was 0.3 plasma transfusion days per 100 admission days (95% CI 0.1 to 0.4, figure 1). Ratios between observed and expected prevalence based on patient-mix ranged from 0.1 to 2.4 across countries (online supplemental eTable 3). This indicates that some countries transfuse more (ratio >1.0) or less (ratio <1.0) than expected. Model specifications for the estimation of the expected prevalences are available in online supplemental eTables 4 and 5 and eFigure 1. Most infants transfused with plasma received their first transfusion in the first days after birth, shown by the steep gradient of the orange line from day 1 to day 7 (figure 2, based on 468 out of 1143 (40.9%) infants followed from birth). By day 7 of life, 9.3% (95% CI 6.6% to 11.9%) of infants had received at least one plasma transfusion, and this proportion increased to 13.5% (95% CI 10.0% to 16.9%) by day 28 of life.

Overall plasma transfusion prevalence. Observed prevalences were calculated using random effects Poisson models to pool the transfusion prevalence per centre into country subgroup estimates and subsequently to derive the overall estimate. Upper limit CIs of Germany and Romania are outside axis limits. Expected prevalence as predicted based on patient-mix using a logistic regression model which included the following variables: sex, gestational age at birth, birth weight, congenital malformations, major bleeding, necrotising enterocolitis (NEC), sepsis, mechanical ventilation, surgical procedure, postnatal day. NICU, neonatal intensive care unit

Cumulative incidence of receiving at least one plasma transfusion during the first 28 postnatal days of life. Adjusted for the competing risks of death and discharge (presented as cumulative incidence, with corresponding 95% CIs) and based on 468 out of 1143 (40.9%) infants followed from birth. Cumulative incidences of plasma transfusion, discharge and death at day 28 of life do not sum up to 100% due to a portion of infants remaining admitted in the neonatal intensive care unit (NICU) without plasma transfusion.
Transfusion indication
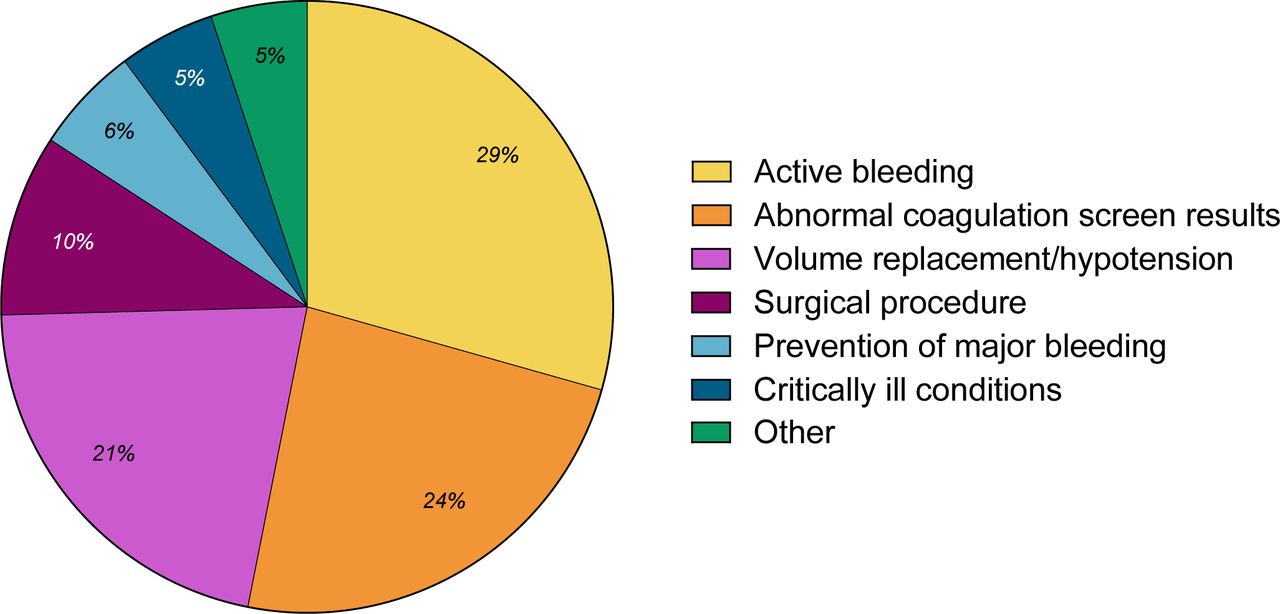
The primary indications for most plasma transfusions were active bleeding (52/177, 29.4%), abnormal coagulation screen results (42/177, 23.7%) or volume replacement/hypotension (38/177, 21.5%) (figure 3). Remaining transfusions were given for surgical procedures (17/177, 9.6%), prevention of major bleeding (10/177, 5.6%), critically ill conditions (9/177, 5.1%) and ‘other’ indications (9/177, 5.1%). ‘Other’ indications included replacement of serum loss (6/177, 3.4%), haematoma (2/177, 1.1%) and oedema (1/177, 0.6%).

Primary indications for 177 plasma transfusions. Indications for transfusion were active bleeding (52/177), abnormal coagulation screen results (42/177), or volume replacement/hypotension (38/177), surgical procedures (17/177), prevention of major bleeding (10/177), critically ill conditions (9/177) and other indications (9/177).
Transfusion volume, duration and infusion rate
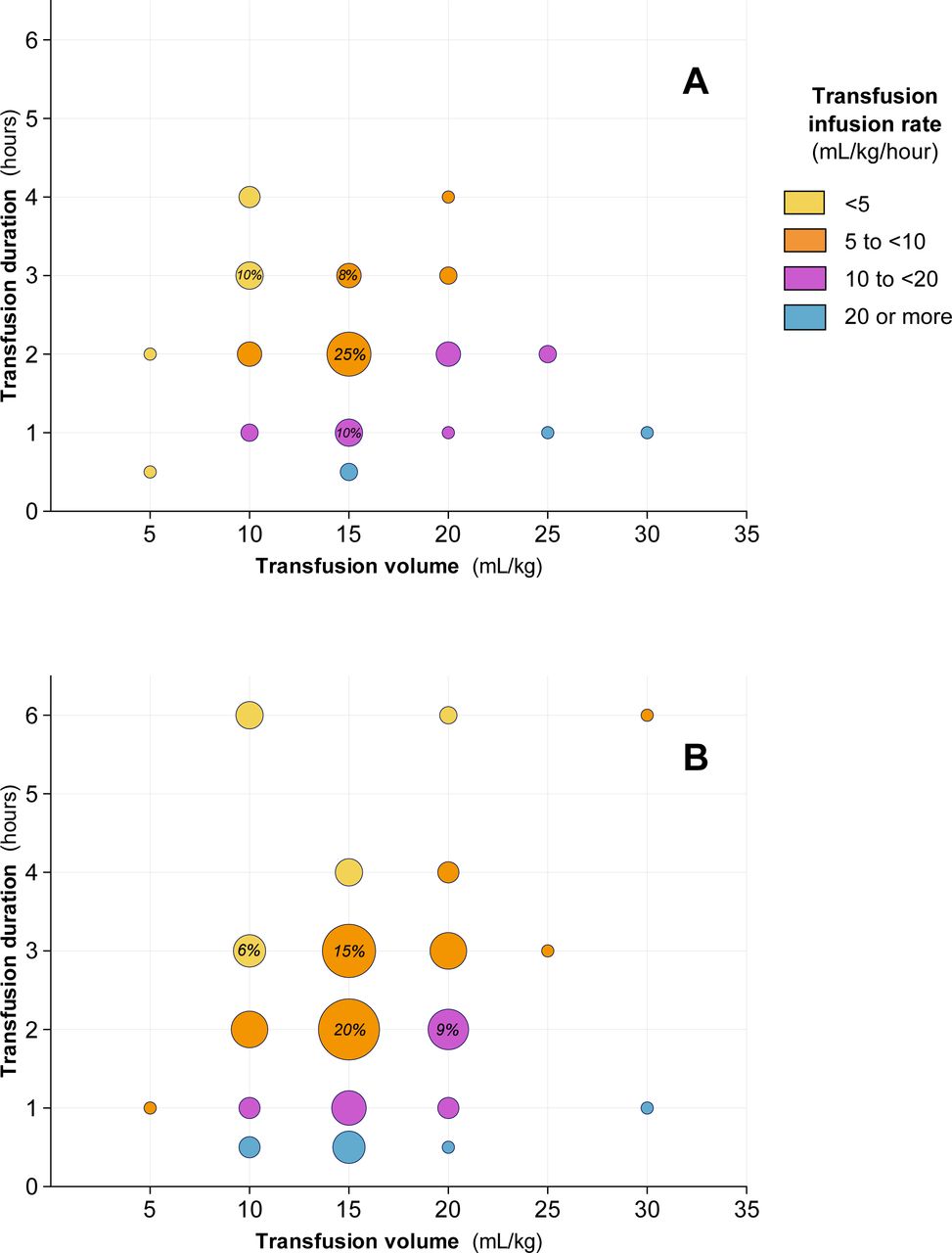
For 176 out of 177 (99.4%) plasma transfusions, volumes ranged from 5 mL/kg to 30 mL/kg, durations ranged from 30 min to 6 hours and infusion rates ranged from below 5 mL/kg/hour to more than 20 mL/kg/hour. The most common volume was 15 mL/kg (88/176, 50.0%), followed by 20 mL/kg in 21.0% (37/176). Most common durations were 2 hours (69/176, 39.2%) and 3 hours (47/176, 26.7%). The most common infusion rate was 5–10 mL/kg/hour (92/176, 52.3%). Transfusion volumes and durations are presented separately for plasma transfusion given for active bleeding and other indications in figure 4A,B, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Transfusion volume, duration and infusion rate of 52 plasma transfusions given for active bleeding. Colours reflect most common infusion rate within each dot, infusion rates of individual transfusions within one dot may vary as infusion rates were calculated using unrounded transfusion volumes and durations. Transfusion volumes were 5 mL/kg or less in 3.9% (2/52), 10 mL/kg in 26.9% (14/52), 15 mL/kg in 46.2% (24/52), 20 mL/kg in 15.4% (8/52), 25 mL/kg in 5.8% (3/52) and 30 mL/kg in 1.9% (1/52). Transfusion durations were 30 min or less in 5.8% (3/52), 1 hour in 19.2% (10/52), 2 hours in 46.2% (24/52), 3 hours in 21.2% (11/52) and 4 hours in 7.7% (4/52). Transfusion infusion rates were 5 mL/kg/hour or less in 19.2% (10/52), 5–10 mL/kg/hour in 46.2% (24/52), 10–20 mL/kg/hour in 26.9% (14/52) and 20 mL/kg/hour or more in 7.7% (4/52). (B) Transfusion volume, duration and infusion rates of 124 plasma transfusions given for other indications than active bleeding. Colours reflect the most common infusion rate within each dot, infusion rates of individual transfusions within one dot may vary as infusion rates were calculated using unrounded transfusion volumes and durations. Transfusion duration and/or volume were unknown in one transfusion (1/125; 0.8%). Transfusion volumes were 5 mL/kg or less in 0.8% (1/124), 10 mL/kg in 21.8% (27/124), 15 mL/kg in 51.6% (64/124), 20 mL/kg in 23.4% (29/124), 25 mL/kg in 0.8% (1/124) and 30 mL/kg in 1.6% (2/124). Transfusion durations were 30 min or less in 8.9% (11/124), 1 hour in 12.9% (16/124), 2 hours in 36.3% (45/124), 3 hours in 29.0% (36/124), 4 hours in 6.5% (8/124) and 6 hours in 6.5% (8/124). Transfusion infusion rates were 5 mL/kg/hour or less in 17.7% (22/124), 5–10 mL/kg/hour in 54.8% (68/124), 10–20 mL/kg/hour in 16.9% (21/124) and 20 mL/kg/hour or more in 10.5% (13/124).
Transfusion-associated adverse effects
We did not record any adverse effects that neonatologists considered related to a preceding plasma transfusion during the study period.
Cryoprecipitate
Only in two of the 22 participating countries did we record the use of cryoprecipitate, with a total of six transfusions. These were primarily indicated for abnormal screen results (5/6) or prevention of major bleeding (1/6). Common volumes were 10 mL/kg (3/6) or 15 mL/kg (3/6), and administration times were 30 min (2/6), 1 hour (1/6) or 2 hours (3/6).
Discussion
Our study is the first to describe plasma transfusion practices across European NICUs. We found significant variability in plasma transfusion practices across the 22 participating countries, including variation in indications, transfusion volumes, duration and infusion rates. Approximately two-thirds of plasma transfusions were given for abnormal coagulation screen results, volume replacement/hypotension and critically ill conditions.
Cumulatively, 13.5% (95% CI 10.0% to 16.9%) of patients received at least one plasma transfusion by day 28 of life, which is slightly higher than previously described in several national studies.4 17–20 The majority of infants that received a plasma transfusion did so during the first week of life. This may be explained by the use of routine coagulation screens after birth or the increased risk of haemorrhage in the first days of life. Additionally, we identified variations in plasma transfusion prevalence across participating countries, which could not be fully explained by differences in patient-mix. National guidelines for plasma transfusions for preterm infants vary considerably from country to country and are often based on limited evidence.21
The primary indication for approximately one in four plasma transfusions was stated to be abnormal coagulation screen results, such as activated partial thromboplastin time or prothrombin time. However, there is no evidence supporting routine transfusion of FFP for non-bleeding neonates to try to correct abnormalities of the coagulation screen alone. Moreover, reliable assessment of coagulation can be more complex in infants. Preterm infants have a different balance of both coagulation factors and natural inhibitors of coagulation.22 23 Although this balance allows healthy infants to maintain adequate haemostasis, the difference in neonatal coagulation factor levels is reflected in longer neonatal coagulation screen results as compared with those of older children and adults.11 17 18 24 However, it is difficult for individual centres to generate their own coagulation reference ranges from preterm infants. As results of coagulation screens are highly dependent on analysers and reagents, published reference ranges may not be directly applicable to local coagulation screen results. In addition, published reference ranges are also often not validated for extreme prematurity.9–12 As a result, neonatal coagulation results may be misinterpreted by clinicians. Additionally, as the effectiveness of plasma transfusions in substantially correcting coagulation abnormalities and reducing bleeding risk has never been conclusively proven in non-bleeding preterm infants, use of plasma for this indication should be approached with caution.2 6 8 This lack of evidence extends to adult intensive care, where the benefit of prophylactic plasma transfusions for non-bleeding patients remains unproven.25 26 Additionally, the haemostatic system of preterm infants may respond different to haemostatic interventions as generally thought. This was evidenced by a large RCT comparing two prophylactic platelet transfusion thresholds.27 Opposite to previous assumptions, the authors found that a liberal platelet transfusion policy resulted in higher rates of mortality and/or major bleeding compared with a restrictive policy. These findings challenge long-held belief in the benefits of prophylactic transfusions and contribute to the ongoing paradigm shift that suggests that the ‘better safe than sorry’ approach should be reconsidered for a ‘less is more’ strategy.28 Future studies should explore factors that influence transfusion decisions and behavioural aspects of clinical decision-making, with the goal of reducing unnecessary transfusions.
Furthermore, bleeding is a multifactorial process influenced by various clinical factors besides coagulation assay results, which should be taken into account when quantifying bleeding risk in infants.22 29 However, accurate prediction of bleeding risk in preterm infants remains a significant challenge. While several risk scoring tools have been developed for adult patient populations, a systematic and validated tool to assess bleeding risk and weigh potential risks and benefits of haemostatic interventions in preterm infants is still lacking.30 Development of a prediction tool that incorporates coagulation assay results, platelet counts and other clinical factors could significantly improve transfusion decision-making for preterm infants by identifying those at high risk of bleeding and weighing risks and benefits of different haemostatic interventions. This approach would be an important step towards individualised transfusion medicine for preterm infants.
Notably, 21% of transfusions were given primarily for volume replacement or hypotension. There is no conclusive evidence supporting use of plasma over other volume replacement options such as crystalloid solutions.31–33 In fact, it is hypothesised that plasma volume expansion can cause pulmonary oedema as a result of increased plasma leakage across capillary membranes.34 35 If volume loss can be adequately replaced by other volume replacement options, it could be argued that these may be preferred over plasma transfusions given their potential risks.
We found wide variation in transfusion dose and durations, both for transfusions given for active bleeding as well as those given for other indications, underlying the absence of evidence for optimal volumes and durations in preterm infants. Although we expected that clinicians might be inclined to administer higher volumes at faster infusion rates in case of active bleeding than in a prophylactic setting, we did not observe this pattern in this study. More evidence is needed to guide optimal administration of plasma for different indications and to minimise variation in practice.
We did not document any adverse effects potentially associated with the plasma transfusions administered, although it is known that plasma transfusion may cause severe complications shortly after administration, such as haemolytic reactions, transfusion-associated circulatory overload or transfusion-related acute lung injury.1 36–38 Plasma transfusion-related adverse events may be overlooked in the context of other recipient comorbidities. Moreover, there may be long-term effects of plasma transfusion that we do not yet know about. There is a developmental mismatch between adult donor blood and neonatal blood, which is also reflected in physiological differences in plasma, with relatively higher concentrations of anti-inflammatory factors in infants.22 39 40 This does not necessarily indicate that the neonatal immune system is impaired, but rather that infants may maintain a highly balanced system adapted to their needs.39 40 Whether transfusion with adult plasma can disturb this balance between proinflammatory and anti-inflammatory factors remains unknown. Our study design did not allow us to assess short- and long-term effects of plasma transfusion in preterm infants, although this is a crucial aspect that warrants further research. Large, high-quality RCTs are needed to substantiate whether plasma transfusions prevent bleeding in preterm infants and should include neurodevelopmental assessments to examine long-term effects. Until then, routine prophylactic plasma transfusions for non-bleeding infants aimed at correcting abnormalities of the coagulation screen alone should generally be avoided.
A limitation of the study is inclusion of a relatively small number of preterm infants per country, which hampers interpretation of results at a national level. Additionally, we did not collect pretransfusion coagulation assay results as these are difficult to interpret due to the lack of standardisation, and therefore we were unable to comment on the degree of abnormality of coagulation results. Lastly, we only collected primary indications for transfusion and did not record any possible secondary indications that influenced clinical decision-making, which could have contributed to our understanding of different transfusion scenarios.
In conclusion, plasma transfusions are often administered to preterm infants in European NICUs despite lack of evidence to guide their use. We observed considerable variation in plasma transfusion practices across Europe, with many transfusions given for indications which are not sufficiently evidence based, such as abnormal coagulation screens without active bleeding or volume replacement. We urgently need evidence-based strategies to guide plasma transfusion use in intensive care for very preterm infants.
Supplemental material
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Medical Research Ethics Committee of the Leiden University Medical Center (G21.207). Thereafter, national or local ethical review boards in the participating centres approved the study. Parents or guardians provided consent where required by national or regional legislation. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The INSPIRE Study Group (non-author collaborators) appears in the Collaborators section. We thank Oliver Karam, Marianne Nellis, Martha Sola-Visner, Amy Keir and Naomi Luban for their advice as members of the study advisory board. This study was initiated in collaboration with the Neonatal Transfusion Network, an international research network focused on generating evidence to improve neonatal transfusion practices.
References
Footnotes
X @fracardo
Contributors Concept and design: NAMH, SFG, KF, HVN, SS, ED, CCR, CD, JGvdB, EL. Acquisition, analysis or interpretation of data: NAMH, SFG, KF, CC-D, MA, AB, KB, FSC, AD, SD, SG, RG, EH, CH, JLK, JM, KM, CMM, TM, MS, TS, GZ, JdJ, NJR, ED, CCR, CD, SlC, JGvdB, EL. Drafting of the manuscript: NAMH, SFG, KF, EL. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: NAMH, CC-D, SlC, JGvdB. Administrative, technical or material support: NAMH, CC-D, MA, AB, KB, FSC, AD, SD, SG, RG, EH, CH, JLK, JM, KM, CMM, TM, MS, TS, GZ, JdJ, NJR, ED, CCR, CD. Supervision: SFG, KF, JGvdB, EL. NAMH and CC-D have directly accessed and verified the underlying data reported in the manuscript. SFG obtained funding. The guarantor is EL.
Funding The study was supported (in part) by research fuding from Sanquin Blood Supply Foundation (PPOC21-08/L2588, RES/00264), the European Blood Alliance (EBA Grant Agreement 2021-02) and the European Society for Paediatric Research (ESPR Post-Doc Research Grant 2020).
Disclaimer The funders of the study had no role in study design, data collection, data analysis, data interpretation or preparation of the manuscript. The contents of this manuscript do not necessarily reflect the views and policies of EBA, nor does mention of tradenames or commercial products constitute endorsement or recommendation of use.
Competing interests SGu disclosed receiving grants from Sanquin Blood Supply Foundation (PPOC21-08/L2588, RES/00264), the European Blood Alliance (EBA Grant Agreement 2021-02) and the European Society for Paediatric Research (ESPR Post-Doc Research Grant 2020). CH and TM disclosed receiving compensation from Sanquin Blood Supply Foundation. JM disclosed receiving compensation from Sanquin Blood Supply Foundation, research grants from Cooperatio and Personmed, and consulting fees from Danone, Nestlé, Baxter and Chiesi. SG disclosed receiving lecture fees from Entegrion, outside this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.